#sociology of medicine
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. is funded by 13 investors.
Text
Compliance, per the two main approaches to medical sociology
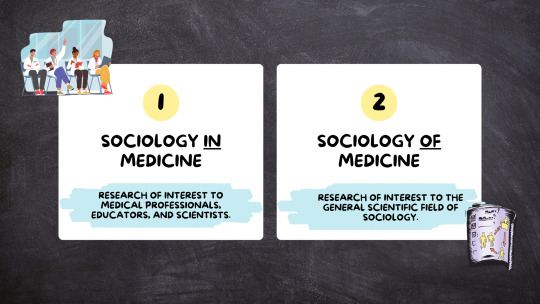
Sociology in medicine is research that’s of interest to medical professionals, medical educators, medical scientists— things that are important to medicine as an institution.
Sociology of medicine tends to be research of interest to the general scientific field of sociology, not only sociologists who study matters of medicine, health, illness, healthcare, and disability. Importantly, it is not that medicine is simply disinterested in sociology of medicine, the institution of medicine sometimes has a vested interest in silencing or arguing against sociology of medicine. Sociology of medicine may not be useful to medical professionals, but if, for example, sociology of medicine is critiquing medical practice, as is often the case, it might move beyond useless to being perceived as offensive.
To further explore the difference between sociology in versus of medicine, let’s take the issue of compliance.

From the medical perspective, patient compliance is vital for successful medical practice and treatment. if your patient is not listening to you–for example, if they’re not taking their medication, and that medication is supposed to get them better, than you are going to have a much more difficult time treating that patient, and thus, a much harder time doing your job, than if the patient “complied” with your treatment plan. Same thing if your patient won’t have surgery. Well, if operating is the way that you do your job and the patient refuses, you cannot do your job as well. So, sociology in medicine would examine compliance with this medical perspective in mind. Sociology in medicine might investigate the barriers to patient compliance, and they might ask about these barriers in terms of patient behavior, asking something like "why are these patients non-compliant?" with the goal of identifying things that can be addressed to help patients better comply, so that medical professionals can have better chances of success when trying to do their jobs.
Now, moving to sociology of medicine—the greater field of sociology is interested in issues of power and inequality. When examining compliance in terms of power and inequality, we might look at something like physician control over patients, which would contribute to areas of sociology beyond medical sociology, such as the larger sociological literature on deviance and social control.
From this perspective, physicians offer something that patients cannot obtain on their own—prescription medications, surgery, imaging…these are all things that are considered both illegal and dangerous when obtained from non-credentialed entities. This means patients must be compliant to avoid severe consequences, like physical injury, disability, or even death. Healthcare providers hold power to help people feel better when they have few, if any, safe alternatives.
Instead of looking at compliance as inherently positive or necessary, we can critique the concept, and most importantly, the continued endorsement of compliance as “positive” and “necessary” by credentialed actors in medicine. So, sociology of medicine, similarly to sociology in medicine, may examine barriers to compliance, but because it does not assume compliance is necessary or helpful to the patient, it leaves room to explore the patient experience. Sociology of medicine can explore things like mistrust of medical professionals, experiences with bias and discrimination in the clinical encounter, and the patient’s understanding of a potential treatment as helpful versus their belief that the treatment is useless (independent of the science on said treatment’s effectiveness).
So, while sociology in medicine and sociology of medicine might both be interested in the question of “why do patients become noncompliant,” sociology in medicine might approach that question with the intent of identifying something that will lead to increased compliance, whereas sociology of medicine may approach the question in terms of medical harm, so not taking the assumption that compliance is positive, instead, taking the more skeptical view that compliance might be an exercise of power on the part of the healthcare provider over the patient and focusing on issues like the potential for patterns of exploitation and/or harm of certain groups of patients with shared characteristics. Sociology of medicine might ask whether healthcare providers, because they are powerful, are inherently good or right. Sociology in medicine would probably not ask this question at all, instead assuming the answer to be "yes"
youtube
#sociology#studyblr#phdblr#social science#medblr#health science#research#paradigm#medical sociology#sociology of medicine#sociology in medicine#compliance#power#inequality#deviance#social control#medical sociology 101#Youtube
3 notes
·
View notes
Text
One of the very few silver linings of winding up with long covid has been experiencing medical care from cardiology.
I have a long history of issues treated by neurology, gastroenterology, and psychiatry. These are fields of medicine that only sorta kinda know what they're doing. Migraines? Only sorta understood. IBS? Even less. Depression? Hahaha yeah right.
And now I'm getting care from cardiology, a medical field that has been built around caring middle-aged men. And holy shit it is a different experience.
There are reliable, valid, and non-invasive ways to measure what's going on with me. Every 3-6 months I get an ECG, an echo, a stand test, and a blood panel to monitor inflammation.
My diagnoses are based on actual measurement, not a doctor's vibes. Treatments have been developed with actual understanding of the relevant etiologies. The drugs I take have actual, measurable impact on the outcome variables of interest. There is clear, measurable improvement of my condition over time. Even though my recovery is going very slowly, I can actually see things are going in the right direction.
Meanwhile my meetings with neurology/psychiatry/GI continue to at best take the approach of "let's throw things at the wall and see what sticks and if you notice it actually helping you". Rheumatology gave up on even trying to help me. Imagine what those fields could do if they had the same level of funding, prestige and scrutiny that medical fields that middle-aged white men care about get.
1 note
·
View note
Text
The ongoing war in Sudan and the ensuing humanitarian crisis has pushed people to the brink. At the borders of conflict zones, selling a kidney is becoming a currency of last resort for people seeking refuge. In June 2023, I managed to contact two young Sudanese women who had fled the fighting in Khartoum. In April 2023, Rania was with her friend Fatima, both students at the University of Khartoum, when the RSF raided the main campus, on the banks of the Nile. “We were trying to hide from the fighting,” Rania told me on the phone. “There were a lot of [female] students there who were afraid to leave. We thought we would be safe, but they found us and forced us to have sex with them.”
Soon after that they packed up their belongings and took a bus heading towards the border with South Sudan. They had heard the route south was cheaper than trying to go north to Egypt, and Rania had a brother living in Kampala, Uganda, whom they hoped to join. It was a seven-day journey from Khartoum to Renk, a small town in South Sudan close to the border where thousands of people had set up temporary camps in bleak conditions. A lack of food, water, healthcare and sanitation had left people at increased risk of disease, malnutrition and violence. There were hundreds of new arrivals each day. “People are crammed together under tarpaulins,” Rania said. “There are mosquitoes everywhere. There’s not enough food, water, soap. Everyone is desperate for assistance. It’s chaos.”
When Rania and Fatima arrived at a makeshift camp on the outskirts of the town, they were approached by soldiers in plain clothes selling tickets for flights from a small airstrip outside Renk to South Sudan’s capital, Juba, and the city of Nimule. The flights, which should form part of the humanitarian corridor, are being controlled by armed militias charging exorbitant fees to board them. “They wanted a lot of money,” Rania said. “The price would go up every day. They said if we didn’t have any money we could have sex with them.”
When they refused, they were told there was something else they could sell: a kidney. “They said that this was the only way we were going to get a flight out of here,” Fatima said. “There were two men who had agreed to this [selling a kidney], but I don’t know what happened to them. I was worried that they would kill me and take my kidney.”
Two weeks after Rania and Fatima first arrived in Renk, they messaged me from Kampala. “We received some money from family members in Uganda. They paid a smuggler $500 to take us to Kampala.” Raina said. “There were no humanitarian agencies or government officials transporting people. The drivers, the militias, they are exploiting people every step of the journey.”
In Renk, they had watched as large trucks carried hundreds of people further south to transit camps that were rumoured to be less crowded and better resourced. Others boarded cramped and overcrowded boats down the Nile to the city of Malakal, from which they would attempt to reach Juba, 970km to the south. Each stage of the journey would come at a cost.
“We are telling you this for a reason,” Fatima said. “We desperately need more support for people trapped in Sudan. In Darfur, there is genocide. But no one is talking about it. Women are being raped every day. Children have been killed and abducted. People are desperate. This is when you sell your kidney.”
— ‘For me, there was no other choice’: inside the global illegal organ trade
#seán columb#‘for me there was no other choice’: inside the global illegal organ trade#current events#medicine#medical ethics#sociology#poverty#exploitation#war#immigration#refugees#human trafficking#organ transplantation#organ trafficking#misogyny#rape#sudanese civil war#war in darfur#sudan#uganda#south sudan#darfur#khartoum#renk#kampala#university of khartoum#rapid support forces#kidneys
45 notes
·
View notes
Text

Vertex, Volume 1/Number 5, Mankind Pub. Co., December 1973
#witches#vertices#occult#vintage#vertex#magazine#sci-fi#mankind publishing company#los angeles#volume one/number five#mankind#science fiction#heinlein#george barr#sidney coleman#gregory benford#december 1973#1973#sociology#medicine#kevin davidson#science
22 notes
·
View notes
Text
Calling all science students and enthusiasts!!
I would absolutely love to have a science-revolving passion project and I’ve narrowed it down to a blog/blog-type-website. I love learning about science but so rarely take the time to actually research the things that interest me. With being a high school student, exams and life this is quite a big task to handle for 1 person and I’d love others to contribute to this!
This is by no means a set plan yet, I’m just sharing a rough idea, so if you could please interact with this post or dm me if you would be interested in something of this kind. Even if you see this 5 months after this was posted (and hopefully a working project or at least WIP) still reach out if you’re interested.
You don’t have to be a great writer for this either nor fascinated about each and every science. My favourite is chemistry, but it would be nice if this project could incorporate the 3 main branches of science: biology, chemistry and physics. It depends on if people would be interested in reading something like this or participating in, and their preferred subjects. You could write about astronomy as a whole, or go into chemistry and analysing electronic configuration, talking about your favourite dinosaur bones in palaeontology, a passive behaviour analysis in psychology, or explaining how exactly scabs work in biology. These would probably be short to mid-length entries and 1/2 times a month.
But this is just my idea and how far I’ve gone with it, feedback is appreciated, there will be more updates to come (not too many until afer my exams in May tho), and I appreciate any reblogs to share this idea with others!
Hopefully a couple people would like to help out in this project and please ask questions if you have any (as a dm or ask) ^^
#studyblr#uni student#university#student#a levels#science#passion project#group project#chemistry#biology#physics#medicine#astronomy#psychology#Sociology#palaeontology#botany#microbiology#toxicology#biotechnology#geology#meteorology#earth science#biochemistry#dark academia#light academia#community project#scienceblr#science blog#the sci journal
118 notes
·
View notes
Text
big question for tumblr girlies
what are your favourite research papers?
#could be on anything#feel free to self promote that brain of yours too<3#research paper#research#literature#stem#studyblr#science#archives#architecture#biology#medicine#history#sociology#psychology#never seen me tag so many actual things lol#law#IT#ecology#environmental science#arts#biomedical engineering#engineering
13 notes
·
View notes
Text
there's this girl in my batch i'm like 90% sure is a communist too (okay well probably not that far left but anywag) i wanna befriend her sooooooooooooo BAD
#we had a sociology and medicine focused lecture in our medical anthropology elective last year#her input was always so solid now we share a look whenever someone says something dumb PLEASEEEE COMMIE TO COMMIE CONVERSATION MAKE IT HAPPE
14 notes
·
View notes
Text
saw that there was a video on tiktok circulating about what people even do with womens studies degrees and I saw a nice little rebuttal video that gave a syllabus list and that’s really nice and informative and all but back to the point there are real jobs that are super important that people can do with humanities degrees and part of fighting the backlash against them is acknowledging they exist
#I mean in a capitalist sense sociology psychology etc are super useful when you’re trying to sell people shit#but like a good chunk of women’s studies is devoted to the political and medical sphere#everything from setting up workplace policies (yes HR more legal)#to studying pay disparities#examining bias in clinical studies#plus there’s the whole research field of doing studies into gender#and the combination of medicine and law like studying anti choice laws etc etc#there are people who do all this shit for a living and it’s all legitimate work
13 notes
·
View notes
Text
Throwback to like three or four years ago when was it when i was on here ranting about how history must be taught better specifically because life is just one big corkboard conspiracy theory except neither conspiracy nor theory, everything is just influenced by everything that happened before and you can't learn about anything without learning about everything that happened before that first. Etc etc.
#i'm actually happy with this i wanted to major in history but knew i didn't have the capabilities for it#this way i got everything i ever wanted. lots of language lots of literature and a decent amount of anthropology sociology and history too#thank God i didn't listen to my folks and study medicine i belong in humanities (my future is crying)
6 notes
·
View notes
Text
In concluding their piece, Lahl and Fell said: 'The authors' suggestion that medical providers should deviate from the principle of 'do no harm' to follow paths where the evidence indicates harm is quite shocking.""This perspective, driven more by ideology, emotions, and personal desires than by evidence, conflicts with the foundations of evidence-based medicine.'
MSU sociology professor Dr. Carla Pfeffer is slammed over scientific journal article saying trans men should be allowed to take testosterone while pregnant, despite warnings hormones may trigger severe health issues in fetuses
Dr. Carla Pfeffer published a paper alongside five other academics concerning the use of testosterone therapy during transgender pregnancy
The sociology professor and her cohorts have since been slammed by two nurses for disregarding the safety of a fetus 'in the name of trans inclusion'
Jennifer Lahl and Kallie Fell hit back at the study, deeming one portion of it 'quite frankly, insane'
By JOE HUTCHISON FOR DAILYMAIL.COM
PUBLISHED: 10:37 EDT, 20 October 2023
A professor has been slammed over a scientific journal in which she said trans man should be allowed to take testosterone while pregnant, despite warnings it could trigger severe health issues.
Dr. Carla Pfeffer, who is not a medical doctor, penned a new paper alongside five other academics titled 'Medical uncertainty and reproduction of the 'normal': Decision-making around testosterone therapy in transgender pregnancy.
Pfeffer, who is a sociology professor at Michigan State University, argues that pregnancy care is too focused on helping women have healthy babies, and that trans men might be fine to take testosterone while pregnant.
The authors , who are sociologists, have since been accused of choosing to disregard the safety of a developing fetus 'in the name of trans inclusion'.
In a scathing response to the paper, two nurses have criticized the article saying if abiding by their take 'would land us in a vacuum devoid of medical ethics'.

Dr Carla Pfeffer, pictured here, published a paper alongside five other academics concerning the use of testosterone therapy during transgender pregnancy

The sociology professor and her cohorts have since been slammed by two nurses for disregarding the safety of a fetus 'in the name of trans inclusion'
Authors Jennifer Lahl and Kallie Fell, who is the Executive Director at The Center for Bioethics and Culture, published a response to the paper titled: 'Is There a Doctor in the House?'
In it, they said: 'The authors argue that 'gendered' pregnancy care is too focused on helping women have healthy babies, and that it might be okay for transmen to continue taking testosterone during pregnancy despite the known health risks to the fetus and effects on its normal development.
'This is, quite frankly, insane.'
In the paper, Pfeffer and her fellow colleagues had studied 70 international trans individuals and 22 health care providers who focus on trans people.
Their paper says: 'We argue that in the context of lacking and uncertain medical evidence (HRT with testosterone during pregnancy and chest feeding) in a highly gendered treatment context (pregnancy and lactation care), both patients and providers tend to pursue precautionary, offspring-focused treatment approaches.'
In response, Lahl and Fell say the findings are flawed as only biologically fertile human females possess the attributes for pregnancy and childbirth.
The two label this 'a simple biological reality', saying that pregnancy care isn't 'gendered' at all.
According to the Mayo Clinic, testosterone may cause birth defects if a pregnant woman comes into contact with it.
Lahl and Fell also added: 'The concerns raised by Pfeffer and colleagues focus on the modern treatment approach physicians take, which they deem excessively 'precautionary' and 'offspring-focused.'

Kal Fell, front, and Jennifer Lahl, background, published a response to the paper titled: 'Is There a Doctor in the House?'
'Fortunately, caring for the child and the mother are neither mutually exclusive nor zero-sum.
'In situations where a woman aspires to become pregnant and commits to motherhood, physicians can provide care that optimizes outcomes for both parties while minimizing potential harm.
'If a woman chooses to continue a pregnancy, doesn't the developing fetus also have a right to the four principles of medical ethics?'
'In such cases, the physician is duty-bound to care for both the child and the mother.'
One health care provider also told researchers: 'I think if you choose to have a pregnancy and your female hormone levels would be already so high that testosterone probably wouldn't even mentally help.
'If you're producing breast milk and you couldn't be without testosterone for mental health, if you couldn't deal without testosterone, then you probably shouldn't be pregnant.'
In concluding their piece, Lahl and Fell said: 'The authors' suggestion that medical providers should deviate from the principle of 'do no harm' to follow paths where the evidence indicates harm is quite shocking.
'This perspective, driven more by ideology, emotions, and personal desires than by evidence, conflicts with the foundations of evidence-based medicine.'
#Dr Carla Pfeffer is a sociology professor#Why is she writing papers on maternal and fetal health?#Jennifer Lahl is speaking the truth#Kallie Fell is speaking the truth#Medical uncertainty and reproduction of the 'normal': Decision-making around testosterone therapy in transgender pregnancy#michigan state university#Pregnancy care is too focused on helping women have healthy babies#statement showing transcult brain rot#The transcult and medical ethics#disregard the safety of a developing fetus in the name of trans inclusion'#Is there a Doctor in the house?#Pregnancy care isn't gendered it's sex based#evidence based medicine
4 notes
·
View notes
Text
"Inclusivity" is not what people claim it is (for their own personal gain)
Lately I'm hearing a lot about inclusivity because people claim that is a good reason for the term "women" or "woman" to disappear from medical pages about female-only health things (while ironically the same thing does NOT happen to men stuff) in favour of being more "inclusive" and "including" trans people. I'm also hearing this a lot in classrooms (I was a teacher and many of my friends still are) when it comes to the inclusivity of people with learning difficulties in normal schools that aren't adapted for learning difficulties. So I thought I'd get some heads out of arses by reminding everyone that is NOT inclusivity.
Let's start by analysing this definition carefully, coming from Cambridge:
Inclusivity is the fact (as in, a thing that is done) of including (grouping together) all types of people (regardless of colour, sex, nationality, sexual orientation, age and so on), things or ideas and treating them all fairly (with fairness) and equally (in the same manner).
Obviously, in real life it gets applied a bit differently, and with limits. We include both girls and boys in a party, but perhaps we set an age limit, we include people with learning difficulties in a classroom where other kids don't have learning difficulties, but we limit the seriousness of those difficulties, and so on. Still, as a general idea, in our society:
Inclusivity is putting both boys and girls in the same classroom, with the same teacher, learning the same things at the same time and treating them equally.
Inclusivity is including (hence the word) LGB under the umbrella of same-sex attraction, as opposed to just saying "gay" and forgetting the rest.
Inclusivity is using the term POC as opposed to simply "black" to include all kinds of people of colour, regardless of whether their actual tone of skin is pitch dark, or whether they're of African descent or another.
Inclusivity is including disabled people into your place of work and helping them to be able to do the same work as their peers.
Let's now pause to think about the part of "treating them all fairly and equally". Notice that "fairly" is put first and given precedence. This is to stress the fact that fairness goes first, and equally refers more to the fact that the fair treatment should put everyone in an equal level of advantage or disadvantage, without giving anyone extra privileges.
Example 1: You've got several children of different heights trying to see over a tall fence. Treating them just equally would mean giving them all the same stool to climb on to look over the fence, even if some kids are already tall enough to see without help, and others might need an extra tall stool. It'd be equal but it wouldn't be fair. But treating them fairly first and equally second means analysing their individual difficulties and giving them each a taller or shorter stool so that in the end their heads are all at equal height over the fence. That way the children end up being treated fairly and being in equal conditions.
Example 2: You bring children with learning difficulties into a school that is not equipped to deal properly with learning difficulties, and where all of the classmates don't have learning difficulties and the teachers aren't trained for them. Sure, it might seem there's inclusivity, because all of the kids are going to the same school regardless of sex, problems, conditions, age, and so on, right? But it isn't, because it isn't fair to the kids with learning difficulties, who will have to reach the same level as their peers without the extra help they need. In this case, they'll also be treated equally, but once again, not fairly. For inclusivity to be done right, you can't forget the fairness, therefore the kids with learning difficulties should be having some accommodations made for them, so that they can be at equal level with their peers, in a fair situation.
Inclusivity is frequently done wrong in schools, hospitals, prisons and all over the world because the principle of fairness gets constantly forgotten, so that we give stools to people who don't need them just because everyone must have one, if you see my point.
Now, ideologies aside, you can't claim inclusivity to remove women's only spaces. A previously "women's only" prison, locker room, bathroom, etc., gets turned into an "everybody" place just for the comfort of trans people, and there is no inclusivity there because it's not fair to anyone and it's not equal to anyone. Think about it. Before each got to have a place of their own, now nobody does, and the reason why there was a division for sex in the first place, which was safety, gets forgotten. Therefore not only there is no fairness and equality and everyone loses a privilege and is forced to be crammed together, but also, it's a total disrespect and slap on the face to for instance victims of sexual assault, whose valid concerns are being disrespected and ignored, and who are being forced to share intimate spaces with people that look like their aggressors, putting them in situations that can be heavily triggering and harmful for their mental health, unfairly.
Why should some people's feelings of safety, fear, concerns, be more valid than others? That's not fair. You want inclusivity? Give them all a private space they don't have to share, where they can all feel safe.
Similarly, there is no inclusivity in removing the term women so that trans women feel better, specially not in medical websites where the term "women" (or its singular, woman) is absolutely essential because all kinds of medical issues, from cancer to heart attacks, can look extremely differently depending solely on biological sex. Because guess what? your health and your body don't give two shits about your gender identity. Neither do medical issues. You can tell yourself you're a woman all you want, but if you were born a boy you won't ever fear cervical cancer, you'll fear prostate cancer, and a heart attack will look different in you than in biological women. And biology cannot be changed no matter how many surgeries you undergo and how many medicines you take. Keeping the terms women and men in medicine and other scientific contexts, to put this example, is for everyone's safety, including yours. And it's inclusive to keep it and exclusive to remove it. Yes, you hear it right, what you've called inclusivity, is actually exclusing half the world's population (women).
And when you hesitate, think about LGBTQ+. Why do we have so many letters? Because inclusivity. The same way you wouldn't want your repressentative letter to disappear from that, because it'd make you invisible, women don't want their noun to disappear from places, because it makes us invisible. And women have historically been invisible long enough.
#invisible women#inclusion#inclusivity#exclusion#exclusivity#society#psychology#sociology#education#biology#medicine#feminism#women#men#women won't wheesht#women's rights#LGBTQ+#queer#lgbt movement#lgbt rights#gays#lesbians#LGB
2 notes
·
View notes
Text
Medical Sociology 101: What is medical sociology, and how is it distinct from other approaches to studying medicine, health, illness, disability, and healthcare?
Medical sociology is both a social science and a health science—it is one of the social scientific approaches to studying topics in health science. So, how is the sociological approach to studying topics in medicine, health, illness, and disability, distinct from other approaches to examining these topics?
Medical sociologists study health, illness, and healthcare, in terms of social problems and social factors. They are not looking at individual issues, nor are they interested in biological or cognitive factors independent of social factors.
Now, it’s important to note that social problems do, in fact, impact individuals, but sociologists aren’t interested in this impact to the individual as much as they’re interested in the shared impacts of social problems across groups of individuals.
So, sociology is not always useful for understanding personal experience; however, sociological research can give insight as to whether your experience is similar to experiences of other people with shared characteristics. instead of asking something like, “why does this individual patient have this experience” the medical sociologist might instead ask, “are there characteristics shared by many patients with this experience which may predispose an individual to have said experience?” So, here, not asking why this individual patient has the experience, but why does this group of patients have this experience while another group does not.
Medical sociology demonstrates that things like likelihood of health or illness, experiences and perceptions of medicine, health, illness, and disability, who provides health care, how healthcare is provided, and to whom it is provided, and institutional aspects of the healthcare system itself, are not random, but instead, are shaped by social factors. Medical problems become social problems when they are shared by many individuals with some similar characteristic, experience, or circumstance.
Watch Here:
youtube
Originally posted on wordpress:
#sociology#education#medical sociology#medical science#medicine#research#science#higher education#open access#free learning#online tutorials#free college lessons#professor#health#disability#healthcare#social science#Youtube
12 notes
·
View notes
Text
First Lady Justice introduces newest Friends With Paws therapy dog at Hinton Area Elementary School | WV News
New Post has been published on https://petn.ws/QfWxt
First Lady Justice introduces newest Friends With Paws therapy dog at Hinton Area Elementary School | WV News
We recognize you are attempting to access this website from a country belonging to the European Economic Area (EEA) including the EU which enforces the General Data Protection Regulation (GDPR) and therefore access cannot be granted at this time. For any issues, contact [email protected] or call 1-800-982-6034.
See full article at https://petn.ws/QfWxt #DogNews #Medicine, #Biology, #Education, #Finance, #Politics, #Psychology, #SchoolSystems, #Sociology, #TheEconomy, #TvBroadcasting, #Zoology
#medicine#biology#education#finance#politics#psychology#school systems#sociology#the economy#tv broadcasting#zoology#Dog News
2 notes
·
View notes
Text
The last needle to be applied against smallpox, before its eradication almost half a century ago, carried a dose of vaccine smaller than a child’s pupil. Four hundred years fit inside that droplet. The devotion of D. A. Henderson’s disease-eradicating team was in it. So were the contributions of Benjamin Rubin and the Spanish boys, as well as the advocacy of Henry Cline and the discovery by Edward Jenner, and before him the evangelism of Lady Montagu, and the influence of Circassian traders from the Caucasus Mountains, who first brought the practice of inoculation to the Ottoman court. An assembly line of discovery, invention, deployment, and trust wound its way through centuries and landed at the tip of a needle. Perhaps there is our final lesson, the one most worth carrying forward. It takes one hero to make a great story, but progress is the story of us all.
— Why the Age of American Progress Ended
#derek thompson#why the age of american progress ended#history#medical history#science#technology#invention#research#medicine#biotechnology#politics#sociology#economics#vaccination#ottoman empire#smallpox#donald henderson#benjamin rubin#henry cline#edward jenner#lady mary wortley montagu
10 notes
·
View notes
Text
What Is Your Dangerous Idea? : Today's Leading Thinkers on the Unthinkable by John Brockman (Editor)
What's Your Dangerous Idea? explores audacious concepts by leading thinkers like Richard Dawkins and Jared Diamond, examining ideas that could significantly impact our lives. Covering diverse topics from medical ethics to existential inquiries.
First published November 6, 2006 Today’s Leading Thinkers Thinking the UnthinkableFrom Copernicus to Darwin, Richard Dawkins to Jared Diamond, Daniel C. Dennett, Brian Greene, Matt Ridley, and Howard Gardner Dangerous IdeasThe world’s leading scientists and thinkers explore bold, remarkable, and dangerous ideas that could change our lives for better or worse. From medical procedures to…
0 notes
Text
[…] “Ross—and he’s clearly not alone—fears that an environment where a significant number of people in no way connected to the left show a spontaneous support for militant and even armed action against what we once would have called “a class enemy” creates an opening for the reconstruction of a left willing to adopt more militant tactics.”
1 note
·
View note